
The bottom line
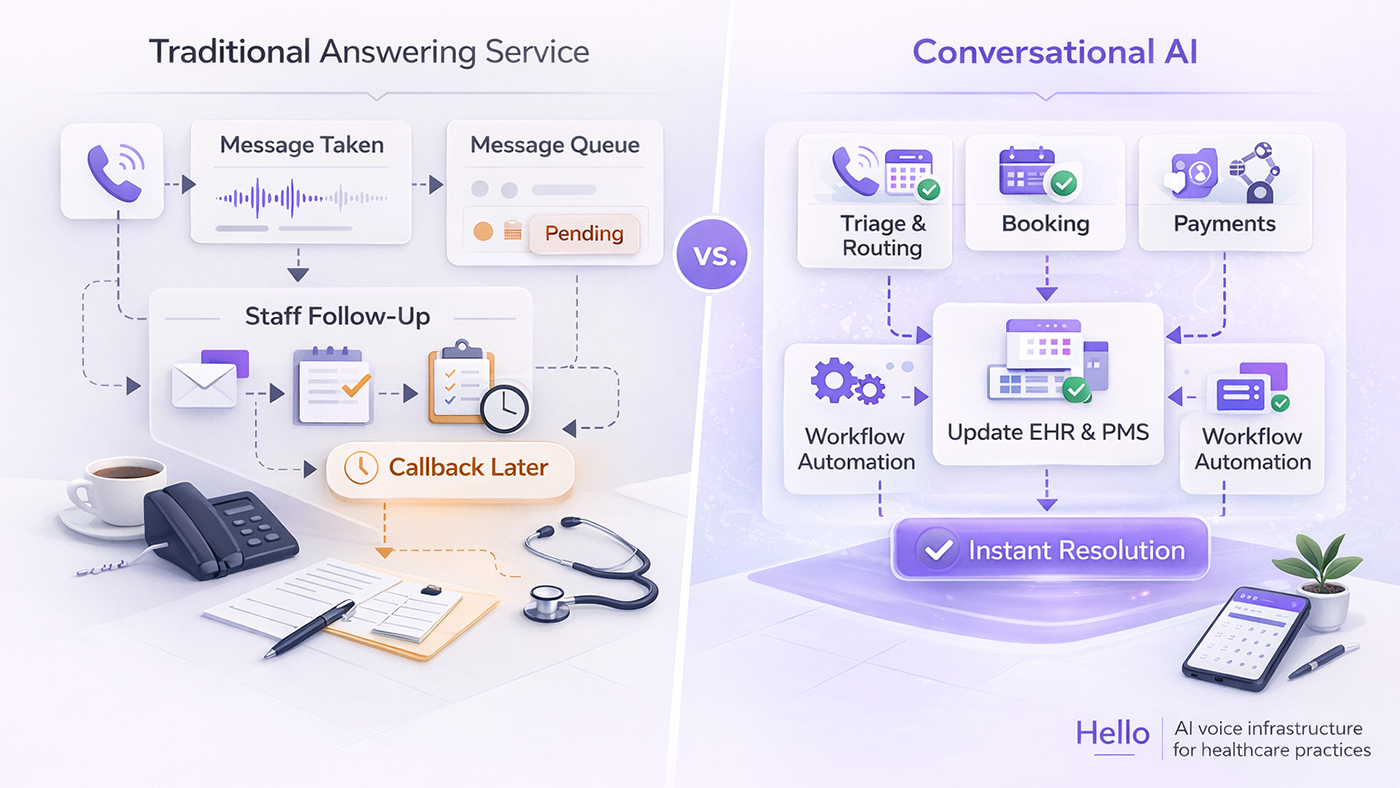
Traditional answering services take messages. AI answering services take action.
A traditional answering service is a staffed call center that writes down what patients say. An AI answering service resolves what patients need: it checks your calendar, books appointments, collects deposits, and logs the interaction in your EHR. One creates a callback list. The other builds tomorrow's schedule while your staff sleeps.
For a practice losing revenue to unanswered or poorly handled calls, this distinction is not semantic. It is operational, and it is measurable.

How a traditional medical answering service works
A traditional medical answering service is a third-party call center. Live operators, located off-site, answer your practice's phone lines during after-hours, lunch breaks, or overflow periods. They follow a predefined script, record a message (patient name, phone number, reason for calling), and relay it to your office via fax, email, or web portal.
This model has served medical practices for decades. It was designed for an era when the alternative was a voicemail box and patients expected a callback the next business day.
What a traditional answering service can do
- Answer the phone with your practice's greeting
- Record the patient's name, number, and reason for calling
- Flag messages as "urgent" or "routine" based on script keywords
- Send the message to your office for next-business-day follow-up
- Page an on-call provider for emergencies (if configured)
What it cannot do
- Check your scheduling system for available appointment slots
- Book, cancel, or reschedule an appointment
- Verify insurance eligibility
- Collect a deposit or copay
- Access patient records for context on repeat callers
- Respond in real-time Spanish without a bilingual operator on that specific shift
- Route calls based on clinical urgency beyond simple keyword matching
The gap between those two lists is where revenue leaks. And for practices handling 200 or more calls per month, the gap is large enough to measure in dollars.
The false sense of coverage
Here is the problem that most practice owners miss: having an answering service feels like coverage. Someone picks up the phone. The patient hears a voice. The practice manager sees messages in the morning. It looks like the system is working.
It is not working. It is documenting its own failure.
Every message slip is a patient who called with intent, whether to book a $4,000 cosmetic consultation, reschedule a post-op follow-up, or pay an outstanding balance, and was told to wait. The answering service did not handle the call. It recorded the fact that nobody handled it.
This is what false coverage looks like in practice:
- A new patient calls at 6:45 PM to book a Mohs surgery consult. The operator writes down a name and number. The patient, anxious about a biopsy result, calls a competitor at 7:02 PM and books there. Your staff never gets the chance to call back.
- A dental patient calls to reschedule a crown prep. The operator cannot access Dentrix or Eaglesoft, so they take a message. Your front desk spends 8 minutes the next morning finding the chart, calling back, and rebooking. Multiply that by 25 reschedule calls per week.
- A patient wants to pay a $350 balance before their next visit. The operator has no access to your billing system. The balance goes unpaid until the patient arrives, creating a checkout bottleneck and an awkward collections conversation.
In each case, the answering service answered the phone. In none of these cases did it resolve the reason the patient called. The practice pays for coverage that covers nothing except the act of picking up.
Traditional answering services cannot automate a single clinical or administrative workflow. They cannot run patient intake. They cannot process payments. They cannot verify insurance. They cannot confirm, cancel, or reschedule appointments. They cannot send post-call confirmations. Every call that requires any action beyond writing a note creates a task that waits for your staff to complete manually, during business hours, competing with walk-ins and today's incoming calls.
This is not a gap in features. It is a structural limitation of the model. A human operator with a script pad and no system access cannot do what a connected AI agent with real-time PMS access does in under 90 seconds.
Six limitations no script can fix
1. The message relay delay
A patient calls your dermatology practice at 7 PM on Thursday. The answering service operator records the message. It reaches your office Friday morning. Your staff calls back at 10 AM. The patient is at work and does not answer. Voicemail. Your staff leaves a message. The patient tries again at 1 PM. Your lines are full. By 5 PM, neither side has connected.
This is not an edge case. It is how the model works. And every failed callback attempt consumes front desk capacity that should handle today's incoming calls. This cycle has a name: the Callback Trap, where returning yesterday's missed calls prevents your team from answering today's new patient inquiries.
2. No scheduling authority
An answering service operator sees a script. They do not see your PMS calendar. When a patient asks, "Can I get a 3 PM slot next Tuesday?", the operator's answer is always the same: "I'll pass that along and someone will call you back."
The patient wanted to book. Instead, they received a promise of a future phone call. For high-intent callers (new patients, cosmetic consultations, urgent referrals), this is often when they call a competitor. Research from Harvard Business Review found that lead contact rates drop by 10x when response time exceeds five minutes. A next-morning callback is a delay measured in hours.
3. No EHR or PMS integration
Traditional services have no connection to your electronic health records or practice management software. Every message is a blank slate. The operator does not know the patient's history, upcoming appointments, insurance status, or outstanding balance.
Your staff then spends the first two minutes of every callback pulling up the chart. Across 30 callbacks per day, that is an hour spent just looking up who called and why. This is one reason dermatology clinics are replacing answering services with systems that access the PMS directly.
4. Limited bilingual support
Approximately 13% of the U.S. population speaks Spanish at home. In Texas, California, and Florida, the share is significantly higher. Traditional answering services may offer bilingual operators, but availability depends on staffing. Coverage gaps are worst on overnight and weekend shifts. Those are also the hours when Spanish-speaking patients are most likely to call.
5. No clinical triage capability
When a dermatology patient calls about a rapidly changing mole, a traditional operator follows the same script used for appointment requests. The message reads "patient has concern about mole." No assessment of urgency. No routing to a clinical nurse line. No flagging for same-day callback.
Dermatology and aesthetic practices handle calls about Mohs surgery scheduling, biopsy anxiety, and $15K cosmetic consultations. Clinical research on patient trust in AI receptionists found that resolution speed and accuracy matter more to patients than whether a human answers. Generic message-taking serves none of these workflows well.
6. The accuracy problem
Traditional answering service operators take messages by hand. They hear clinical terms through phone audio and write down what they think they heard. "Metformin" becomes "Metformen." "Dr. Bhattacharyya" becomes "Dr. B." "Mohs micrographic surgery" becomes "skin surgery." A patient spelling out "Juvederm Voluma XC" gets recorded as "filler injection."
Your staff then spends time deciphering handwritten or hastily typed messages, correcting patient names in the EHR, and clarifying medication details before they can act on anything. Every inaccurate message adds friction. Enough of them, and your team stops trusting the messages entirely. They call every patient back regardless of what the note says, because the note is unreliable.
AI captures everything digitally. Medical NLP trained on clinical terminology transcribes "Mohs micrographic surgery" correctly the first time. Patient names are captured with exact spelling, confirmed during the call. Medication names map to validated drug databases. The transcript is searchable, auditable, and accurate, not a handwritten slip with a question mark next to a drug name your staff has to Google.
What an AI answering service does instead
An AI answering service replaces the message-relay model with a resolution model. The phone rings once, maybe twice. The AI picks up. No hold queue. No "please hold while I transfer you." The patient is speaking to a system that already has access to your calendar, your patient records, and your scheduling rules.
Within 60 to 90 seconds, the call is resolved. Here is what the AI handles during a single patient call:
Scheduling and appointments
- Checks your PMS/EHR calendar in real time for available slots
- Books, cancels, or reschedules appointments during the call
- Follows your practice's specific scheduling rules (provider preferences, procedure durations, buffer times)
- Sends the patient a text confirmation before they hang up
Patient intake
- Collects new patient demographics, medical history, and insurance information over the phone
- Writes structured intake data directly into your EHR, not as a free-text note, but as discrete fields your clinical staff can act on
- Handles pre-visit questionnaires and consent acknowledgments
For a detailed walkthrough of how AI voice agents automate each step of the intake process, including EHR write-back and insurance verification, see how AI voice agents improve patient intake.
Payments and deposits
- Collects deposits at time of booking to reduce no-shows
- Processes copay and outstanding balance payments over the phone
- Records payment confirmations in the patient record
Routing and triage
- Routes clinical concerns to the appropriate staff member based on configurable urgency rules
- Flags calls that require human judgment with full context (transcript, patient info, detected intent)
- Logs every interaction in your EHR with structured data and a searchable transcript
The patient hangs up with a booked appointment, a payment confirmation, or a clear next step. Your staff arrives in the morning to a schedule that was built overnight, intake forms already in the system, deposits already collected. No message slips. No callback list.
The economic difference is measurable. Traditional services charge $0.75 to $1.50 per minute of operator time. An AI answering service uses fixed monthly pricing that does not spike during high-volume periods. When you need the system most (Monday mornings, after long weekends, flu season), it does not cost more.
Monday morning: chaos vs. clarity
This is the difference practice managers feel in their body at 8 AM every Monday.
With a traditional answering service
Your front desk arrives to a stack of message slips from the weekend. Some are handwritten. Some are printed from the portal. A few are illegible. Each slip is a task: call back this patient, look up that chart, verify this insurance, book that appointment, collect this copay. Twenty-three messages from Saturday and Sunday. Twenty-three open loops. Your first hour of the week is phone tag with patients who called two days ago, while today's patients are checking in at the window and today's phones are already ringing.
The answering service gave you a report of work to do.
With an AI answering service
Your front desk arrives to a dashboard. Fourteen appointments booked over the weekend. Three deposits collected ($1,200 in revenue captured before anyone clocked in). Two insurance verifications completed. One clinical concern flagged for Dr. Smith with a full transcript and the patient's chart already pulled up. The Monday morning briefing takes four minutes. It is a status report, not a to-do list.
The AI gave you a report of work already completed.
Traditional answering services create Monday morning chaos. AI creates Monday morning clarity. That contrast repeats every evening, every weekend, every holiday your practice is closed. Over a year, it compounds into thousands of hours your staff either spends on catch-up callbacks or does not have to.
Head-to-head comparison
| Capability | Traditional | AI Answering Service |
|---|---|---|
| Response time | Varies (hold queue, often 30+ seconds) | 1-2 rings, no hold queue |
| After-hours coverage | Message-taking only | Full-service (booking, intake, deposits, routing) |
| Scheduling authority | None (message relay) | Real-time PMS booking, cancellation, rescheduling |
| Patient intake | Not available | Full intake: demographics, history, insurance, consent |
| Payment processing | Not available | Deposits, copays, outstanding balance collection |
| EHR/PMS integration | None | Native (Dentrix, Eaglesoft, Open Dental, Nextech, ModMed) |
| Workflow automation | Zero (every call generates manual staff work) | End-to-end (booking to confirmation to EHR entry) |
| Bilingual support | Depends on staffing | Native English + Spanish, every call |
| HIPAA compliance | Varies by vendor | BAA required, encryption at rest and in transit |
| Cost model | Per-minute ($0.75-$1.50/min) | Fixed monthly |
| Concurrent call capacity | Staff-constrained | Elastic (unlimited concurrent) |
| Patient data capture | Free-text message pad | Structured EHR entry with call transcript |
| Message accuracy | Handwritten, error-prone (misspelled names, medications, procedures) | Digital capture with medical NLP, verified clinical terminology |
| Morning staff workload | Full callback list requiring manual processing | Completion report (appointments booked, deposits collected, concerns flagged) |
Comparison notes:
- Traditional answering service capabilities reflect industry-standard offerings from companies such as Ruby, AnswerConnect, and MAP Communications. Individual vendor capabilities may vary.
- AI answering service capabilities reflect enterprise-grade platforms with native PMS integration. Not all AI answering services offer the full feature set listed above. Verify integration depth before committing.
- Per-minute pricing ranges are based on published rates from major medical answering service vendors (2025-2026). Actual rates depend on call volume, contract terms, and after-hours premiums.
Is an AI answering service safe for healthcare?
Patient phone calls contain protected health information (PHI). Any service handling those calls, whether human or AI, must meet HIPAA security requirements. The compliance mechanisms differ between the two models.
What to verify before choosing any answering service:
- Does the vendor sign a Business Associate Agreement (BAA)?
- Is call data encrypted in transit and at rest?
- Are there immutable audit logs for every patient interaction?
- What is the data retention and deletion policy?
- For practices treating substance use disorders: does the system comply with 42 CFR Part 2 requirements?
A BAA alone is not sufficient. Real security infrastructure for an AI receptionist requires encryption at the conversation layer, SOC 2 Type II auditing, and access controls that cover the AI model itself. If a vendor says "HIPAA compliant" but cannot produce a BAA on request, that is a red flag.
When a traditional answering service still makes sense
Not every practice needs an AI answering service. Traditional services may still fit practices that:
- Handle fewer than 50 calls per month and primarily need emergency paging
- Operate in contexts where every call requires human judgment (certain psychiatric or crisis-line settings)
- Are in the middle of an AI implementation and need bridge coverage
For practices handling 200+ calls per month with scheduling, intake, or payment workflows, the economics and patient experience both favor AI.
How to evaluate an AI answering service
Before signing with any AI answering service vendor, ask these questions:
- Can I hear a live demo call using my practice's greeting and scheduling rules?
- Which PMS/EHR systems does it integrate with? (Ask specifically about your system: Dentrix, Eaglesoft, Open Dental, Nextech, ModMed, drchrono.)
- What happens when the AI encounters a call it cannot resolve?
- How long does implementation take, and what does the first 30 days look like?
- Is there a BAA? Can I review your security documentation?
- How do you handle bilingual callers?
- "HIPAA compliant" with no BAA available on request
- No PMS integration (just a "smart voicemail" that still requires staff callbacks)
- Per-minute pricing with no cap, meaning costs spike during your highest-volume periods
- No live demo available
- No clear escalation path for calls the AI cannot handle
FAQ
Can an AI answering service handle complex scheduling like Mohs surgery or multi-visit treatment plans?
Yes. AI answering services configured for dermatology, dental, and aesthetic medicine handle multi-step scheduling, including pre-authorization workflows and deposit collection. The system follows your practice's specific scheduling rules, not a generic script.
What happens when the AI cannot resolve a call?
During business hours, the call transfers to your staff in real time. After hours, the AI flags the call for priority follow-up with full context (transcript, patient info, intent), so your team starts the next morning with everything they need to resolve it.
How long does implementation take?
Most single-location practices go live in 7 to 10 business days. This includes PMS integration, voice configuration, scheduling rule setup, and testing. Multi-location practices typically need 2 to 4 weeks. See Hello's implementation tiers for specifics on what each level includes.
What is the "false sense of coverage" with a traditional answering service?
It means someone answers the phone, but nothing gets done. The operator takes a message. Your staff still has to call back, look up the chart, book the appointment, collect payment, and complete intake. The answering service creates the appearance of coverage while generating a backlog of manual work that competes with today's live patients. Practices often do not realize this until they track how many after-hours callers actually convert to booked appointments. For most practices using traditional services, that number is close to zero.
Can an AI answering service handle patient intake over the phone?
Yes. AI answering services collect new patient demographics, medical history, insurance information, and consent acknowledgments during the call. The data writes directly into your EHR as structured fields, not as a free-text message that your staff has to re-enter manually the next morning.
Do traditional answering services make errors in their messages?
Frequently. Operators hear clinical terms through phone audio and transcribe them by hand. Patient names, medication names (Metformin recorded as "Metformen"), and procedure names (Mohs micrographic surgery recorded as "skin surgery") are commonly misspelled or abbreviated beyond recognition. AI answering services use medical NLP trained on clinical terminology to capture names, medications, and procedures accurately in a searchable digital transcript.
What does Monday morning look like with an AI answering service compared to a traditional one?
With a traditional service, your staff arrives to a stack of message slips that are all tasks: call back patients, look up charts, verify insurance, book appointments. With an AI answering service, your staff arrives to a completion report: appointments already booked, deposits already collected, insurance already verified, and clinical concerns flagged with full context. The morning briefing takes minutes instead of hours.
AI answering services will replace traditional message-taking in healthcare. The only question is how much revenue your practice loses before you make the switch.